
Your Shoulder's Been Lying to You: The Truth About Rotator Cuff Injuries in Singapore
Mar 15, 2026
You reach up to grab something from the top shelf, and there it is — that familiar twinge deep in the front of your shoulder. Or maybe it's the dull ache that wakes you up when you roll onto your side at night. Or the unsettling weakness you feel trying to lift your laptop bag. You've been managing it for weeks, maybe months. You've Googled your symptoms, and the word "rotator cuff" keeps coming up.
Then you see a specialist. They confirm it. And before you know it, words like "tear", "decompression", and "surgery" are on the table.
If that sounds familiar, this article is for you — because there is a lot about rotator cuff injuries that the surgical referral pathway doesn't always communicate clearly, and understanding the full picture could save you months of unnecessary anxiety, expense, and recovery time.
At Back in Health Osteopathy Singapore, rotator cuff injuries are one of the most common shoulder conditions we treat. In this guide, we'll walk you through what's actually happening in your shoulder, why so many cases are misunderstood, and how an osteopathic approach can help your shoulder recover — even if you've been told surgery is inevitable.
What Is the Rotator Cuff, and Why Does It Get Injured So Easily?
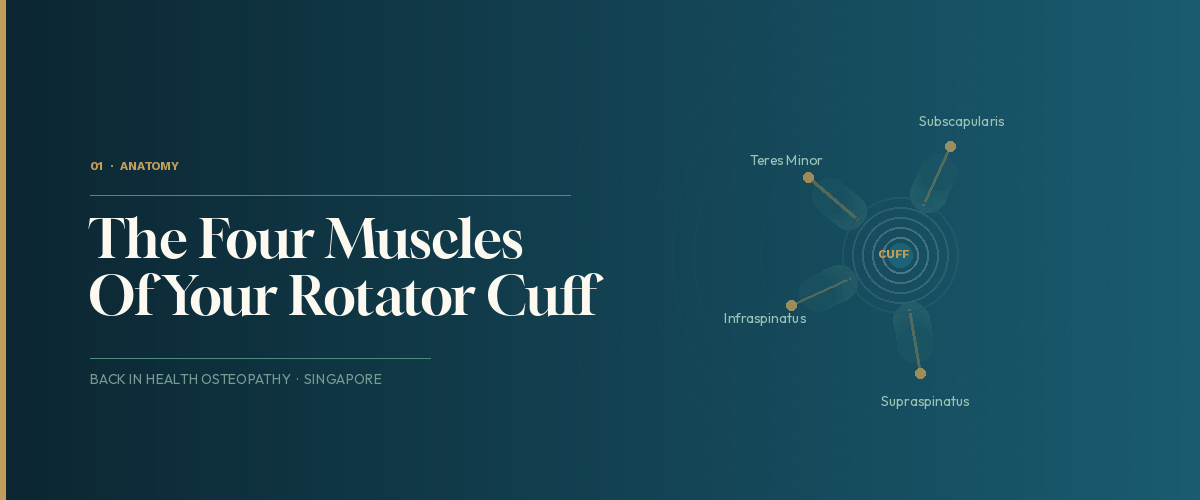
The rotator cuff isn't a single structure — it's a group of four muscles and their tendons that wrap around your shoulder joint like a cuff around a shirt sleeve. These four muscles — the supraspinatus, infraspinatus, teres minor, and subscapularis — have one critical job: to keep your upper arm bone sitting firmly and correctly inside the shallow socket of your shoulder, while also allowing it to rotate and lift in virtually every direction.
That's a complex, high-demand task. And in Singapore's work environment — long hours at a desk, overhead activities in the gym, sports involving throwing or overhead movement, or simply the repetitive strain of daily tasks — the rotator cuff is under near-constant load.
The most common causes of rotator cuff problems include:
Degeneration over time. The tendons of the rotator cuff have a relatively poor blood supply compared to muscles, which means they repair slowly. Decades of use gradually weaken the tendon fibres. This is why rotator cuff issues become much more common over 40 — not because something dramatic happened, but because years of small stresses have accumulated.
Repetitive overhead activity. Swimmers, tennis players, volleyball players, painters, and anyone who spends long periods with their arm raised above their head are at elevated risk. Even hanging laundry outside can contribute to the cumulative load over time.
Posture and shoulder mechanics. This is the part that rarely gets discussed in orthopaedic consultations: poor upper back and shoulder blade positioning can dramatically reduce the space that the rotator cuff tendons move through, causing them to be pinched or compressed on every arm movement. This is called shoulder impingement, and it's often the root cause of the injury — not the injury itself.
Acute trauma. A fall onto an outstretched arm, a sudden pull or lift, or a direct impact to the shoulder can cause an immediate tear. This type of rotator cuff injury presents differently — with intense, immediate pain and sudden loss of strength.
The Diagnosis That Sounds Worse Than It Is

Here's something that surprises many of our patients: you can have a rotator cuff tear on an MRI scan and feel absolutely no pain whatsoever.
This is not a fringe observation. Research has shown that rotator cuff tears are found in a significant portion of people who have never reported any shoulder symptoms. Tears appear to be much more common in older populations — up to two-thirds of people in their 60s may have rotator cuff changes visible on imaging that cause them no discomfort or functional limitation at all.
This matters enormously for how you interpret your diagnosis.
A rotator cuff tear on an MRI is a finding. It is not automatically a sentence. The critical question is not "do I have a tear?" but "is this tear responsible for my symptoms, and if so, what is the best way to address it?"
The answer to that second question is almost always: start with conservative management.
Even the most surgery-oriented specialists acknowledge that non-surgical treatment should be the first line of care for the majority of rotator cuff injuries. In most cases, patients find meaningful improvement in pain and function through conservative approaches — without surgical repair of the underlying tear.
Why the Shoulder Is Never Just a Shoulder Problem

This is where osteopathic thinking really earns its place.
Most rotator cuff treatment focuses exclusively on the shoulder itself — stretching, strengthening, injections, or surgery. The problem with this approach is that the shoulder doesn't work in isolation. It is part of an interconnected system that includes the neck, the upper thoracic spine, the shoulder blade, and the ribcage. When any part of that system is restricted or poorly coordinated, the rotator cuff pays the price.
Consider a few common patterns we see at Back in Health:
The stiff upper back. When the thoracic spine (mid-back) is restricted and doesn't extend or rotate freely, the shoulder blade cannot move through its full range of arm elevation. This compresses the suproacromial space — the tunnel your rotator cuff tendons run through — on every lift of the arm. The tendons get repeatedly pinched, become irritated, and over time can fray and tear. Treating the shoulder alone while ignoring this thoracic restriction is like treating a blister without addressing the ill-fitting shoe causing it.
The tight chest. Prolonged desk work shortens the pectoralis minor — the small muscle that runs from your chest to the tip of your shoulder blade. When this muscle is chronically tight, it tilts the shoulder blade forward and downward, again reducing the space for the rotator cuff tendons. This is one of the most common postural contributors to shoulder impingement in Singapore's office population, and it's almost never addressed by the time a patient arrives in the orthopaedic system.
Neck involvement. The nerves that supply the shoulder and arm originate from the cervical spine (neck). When the neck has restricted movement or joint compression, it can produce referred pain into the shoulder that mimics rotator cuff pain — and it can also reduce the efficiency of nerve signalling to the rotator cuff muscles, making them weaker and more vulnerable to injury.
A thorough osteopathic assessment looks at all of these relationships. We treat what is actually driving the problem, not just where it hurts.
How Osteopathy Treats Rotator Cuff Injuries

An osteopathic approach to rotator cuff injury is systematic, hands-on, and built around restoring normal movement throughout the entire shoulder complex — not just the joint itself.
Here's what treatment typically involves at Back in Health Osteopathy Singapore:
Thoracic and cervical spine mobilisation. Restoring movement to the upper and mid-back is often the single most impactful early intervention for shoulder impingement. Research has shown that thoracic spine manipulation produces statistically significant improvements in shoulder pain and range of motion — often immediately following treatment. It's one of the most underutilised tools in shoulder rehabilitation.
Soft tissue work and myofascial release. We address the muscles that are maintaining the dysfunctional pattern — particularly the pectoralis minor, upper trapezius, and the rotator cuff muscles themselves. Reducing tension in these structures creates space and allows the shoulder mechanics to begin normalising.
Shoulder joint mobilisation. Gentle, targeted movements of the glenohumeral joint (where the arm meets the socket) restore glide and rotation, reduce pain, and improve the joint's ability to receive load again.
Dry needling. Back in Health also offers dry needling, which can be particularly effective for deactivating the trigger points that commonly develop in rotator cuff injuries — especially the deep supraspinatus and infraspinatus muscles, which are difficult to reach with surface massage alone. Many patients notice a marked release in shoulder tension and an improved range of motion following dry needling sessions.
Exercise rehabilitation. This is non-negotiable in rotator cuff recovery. We prescribe targeted strengthening for the rotator cuff muscles — particularly the infraspinatus and teres minor, which are chronically underloaded in most patients — alongside scapular stabilisation work to retrain the mechanics of the shoulder blade. Exercises are progressed systematically as the shoulder tolerates increased load.
Shockwave therapy. For cases involving calcific tendinopathy (calcium deposits in the rotator cuff tendons) or chronic tendon degeneration that is slow to respond, Back in Health's shockwave therapy can accelerate tissue healing and significantly reduce pain. It is particularly effective for stubborn cases that have plateaued with manual therapy and exercise alone.
What You Can Do Right Now
While professional treatment makes a significant difference, there are practical steps you can take today to reduce load on your rotator cuff:
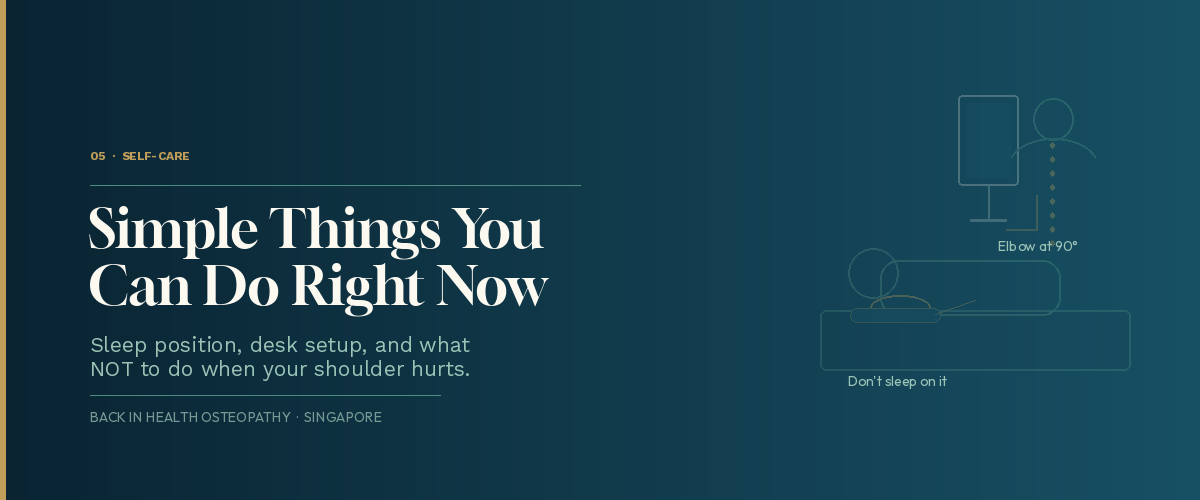
Stop sleeping on the affected shoulder. Sleeping with the arm compressed under your body or lying on the injured shoulder creates hours of sustained pressure on already-irritated tendons. Try sleeping on your back or on the opposite side with the affected arm resting on a pillow in front of you.
Avoid the specific movements that provoke pain. This sounds obvious, but many people continue to load the painful shoulder in the hope it will "work itself out." Repeated provocation delays healing. If reaching overhead hurts, modify the task or the height. If certain pressing or pulling movements aggravate it, stop or modify them.
Check your desk setup. If you use a mouse, ensure your arm is not reaching forward or to the side for extended periods — this position loads the supraspinatus continuously. Your keyboard and mouse should be close to your body, with your elbow roughly at 90 degrees.
Work on your upper back mobility. Sit at the edge of a chair, place your hands behind your head, and gently extend your upper back over the back of the chair. Do this 10 times, several times a day. Improving thoracic extension is one of the most effective things you can do at home for shoulder impingement, and it costs you nothing.
Don't stretch into pain. Many people aggressively stretch a painful shoulder, believing that tightness is the main problem. Overstretching an already irritated and potentially torn structure can worsen symptoms. If you want to work on shoulder mobility, do it gently and only in ranges that are comfortable.
When Should You See an Osteopath?
We recommend booking an assessment if any of the following apply:
- Shoulder pain has been present for more than two weeks and isn't clearly improving
- You have pain reaching overhead, behind your back, or when lifting your arm to the side
- Pain wakes you at night or prevents you from sleeping on one side
- You've noticed weakness in the shoulder — difficulty lifting objects that were previously easy
- You've been told you have a rotator cuff tear, and you want to explore conservative management before considering surgery
- You've already had surgery and are not recovering as expected
It's also worth noting that the earlier you address a rotator cuff injury, the better the prognosis. Chronic, long-standing injuries that have been compensated for years take longer to resolve than more recent problems caught early.
A Word on Surgery
Surgery for rotator cuff tears is sometimes necessary — particularly for complete tears in younger, active individuals or for cases that have genuinely failed a proper trial of conservative management (typically defined as 12 weeks of adequate rehabilitation).
However, the evidence also shows that for many presentations — especially partial tears and tendinopathy — the outcomes of surgery and conservative management are comparable at 12 months. The decision to pursue surgery should be made with a full understanding of the alternatives and ideally after a genuine attempt at rehabilitation, not as a first response to a finding on an MRI.
If you've recently had a rotator cuff diagnosis and surgery has been mentioned, we would strongly encourage you to get a full assessment and try a course of conservative care first. You can always choose surgery later. You cannot un-have it.
Ready to Get Your Shoulder Properly Assessed?
If you're dealing with shoulder pain, a rotator cuff diagnosis, or persistent weakness and stiffness that isn't resolving on its own, the team at Back in Health Osteopathy Singapore is here to help.
We take the time to assess the whole picture — your shoulder, your spine, your posture, and your daily demands — and create a treatment plan that addresses why you're in pain, not just where.
📍 Book your appointment today at www.backinhealth.com.sg/bookings
Don't put it off. Rotator cuff injuries that are caught and managed early respond far better than those left to become chronic. Let us help you get your shoulder back to full strength.
Back in Health Osteopathy Singapore offers osteopathy, IDD therapy, shockwave therapy, dry needling, and clinical pilates. To learn more about our services or to book an appointment, visit www.backinhealth.com.sg.
This article is for general informational purposes only and does not constitute medical advice. If you are experiencing shoulder pain or have been diagnosed with a rotator cuff injury, please consult a qualified healthcare practitioner for an individualised assessment and treatment plan.
