
Why Your Knee Hurts When You Run — And How to Fix It
Apr 22, 2026
You've been building up your mileage nicely. The Sundown Marathon is on the calendar. You've got your route, your shoes, your playlist. Then one morning, you feel it — a dull, grinding ache behind your kneecap that flares on the downhill stretch of your morning run, gets worse on the MRT stairs, and refuses to let you sit through a meeting with your knee bent.
Welcome to runner's knee.
It's the most common running injury we see at Back in Health Osteopathy Singapore, and it comes with a frustrating paradox: rest makes it feel better, but the moment you start running again, it's back within a kilometre. If that sounds familiar, this post is for you — because runner's knee is rarely solved by simply resting. And it's rarely just about your knee.
What Is Runner's Knee?
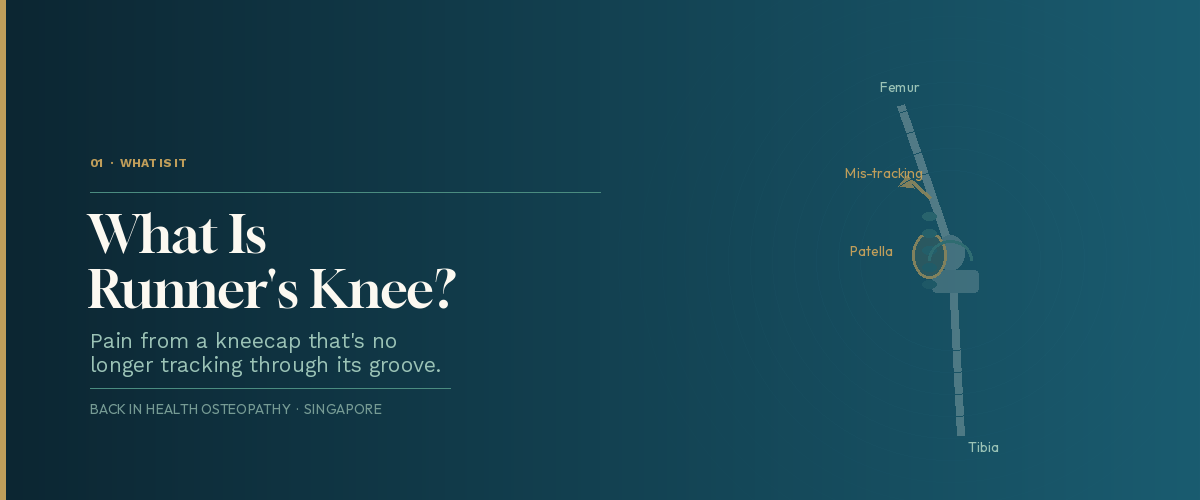
Runner's knee is the colloquial name for patellofemoral pain syndrome (PFPS) — pain at the front of the knee, around or behind the kneecap (patella), that typically develops with activity and persists or worsens without proper treatment.
The kneecap isn't fixed. It glides up and down a groove at the end of your thigh bone (femur) every time you bend and straighten your leg. When it tracks cleanly through that groove, you feel nothing. When it tracks incorrectly — pulled to one side, tipped forward, or grinding rather than gliding — the cartilage and surrounding tissue become irritated, inflamed, and painful.
The name "runner's knee" is slightly misleading. While running is the most common trigger, PFPS affects cyclists, gym-goers, hikers, and anyone who regularly climbs stairs or squats. If you're spending your Sunday doing the Bukit Timah trails or your evenings at F45, you're just as susceptible as a marathon runner.
How to Know If It's Runner's Knee

The hallmark symptoms of patellofemoral pain syndrome are fairly distinctive:
Pain around or behind the kneecap — typically felt at the front of the knee, either directly over or surrounding the patella. It can feel like a dull ache, a burning sensation, or occasionally a sharper pain during high-load movements.
The "theatre sign" — stiffness and pain after sitting for a prolonged period with your knees bent. After a long flight, a two-hour movie, or an afternoon at your desk, standing up feels stiff and uncomfortable for the first few steps. This is a classic PFPS presentation, and many people don't initially connect it to a running injury.
Pain going down stairs or downhill — descending puts significantly more compressive force through the patellofemoral joint than ascending. If your knee complains loudly going downstairs but is quieter going up, runner's knee is a likely culprit.
Pain that worsens progressively during a run — you might feel fine for the first 5–10 minutes, then notice a growing ache that builds over distance and forces you to slow down or stop.
Occasional grinding or clicking — not always present, but some people notice a sensation of crunching or catching in the knee during movement.
It's worth noting what runner's knee typically doesn't involve: significant swelling, locking of the joint, or giving way. If you're experiencing any of those, book an assessment promptly — it may indicate a different structural issue that needs specific investigation.
Why Your Knee Keeps Hurting — The Real Cause Most People Miss

Here's the thing that most online articles about runner's knee don't tell you clearly enough: the problem is almost never in the knee itself.
The kneecap is the messenger. The real issue is upstream.
When the muscles above the knee — particularly the gluteus medius, gluteus maximus, and hip external rotators — aren't doing their job properly, the entire lower limb loading pattern changes. The thigh rotates inward during each stride, the knee collapses slightly toward the midline, and the patella is dragged out of its groove on every step. Over thousands of steps per run, the result is the relentless friction and irritation that produces PFPS.
Research supports this clearly. Studies have found that people with patellofemoral pain syndrome show reduced activation of the gluteus medius and gluteus maximus compared to pain-free runners, and that greater hip adduction angles during running are associated with increased risk of developing the condition. The current clinical guidelines for PFPS — updated as recently as 2025 — specifically recommend hip and core strengthening as the primary rehabilitation focus, rather than isolated quadriceps exercises.
This is where the traditional approach to runner's knee falls short. Taping the patella and doing quad sets doesn't address why the kneecap is tracking badly. It manages symptoms without fixing the source.
An osteopathic assessment looks at the whole chain: how your foot strikes the ground, how your ankle moves, how your hip functions through its full range, how your pelvis is positioned, whether your thoracolumbar fascia and lower back are contributing to altered movement patterns. Often, runners with PFPS also have a stiff hip flexor, a tight IT band, or restricted lumbar spine mobility that creates a cascade of compensation all the way down to the kneecap.
Fix the chain. The knee follows.
The Most Common Drivers We See at Back in Health
In our clinic, the runners who come to us with patellofemoral pain typically have one or more of the following underlying contributors:
Weak hip abductors and external rotators. The gluteus medius in particular is the critical stabiliser of the pelvis and femur during single-leg stance — which is what every running stride is. When it's underactivated or weak, the femur drops and internally rotates on each footfall, pulling the patella out of its groove. This is extremely common in desk-bound Singaporeans whose glutes are chronically underloaded from prolonged sitting.
Tight quadriceps and hip flexors. If the quad (specifically the vastus lateralis) is chronically tight, it pulls the patella laterally and increases compressive force on the outer edge of the joint. Tight hip flexors from long hours at a desk also tilt the pelvis forward, altering the angle at which forces are transmitted through the knee during running.
A stiff ankle or foot. Restricted dorsiflexion (the ability of the ankle to bend your shin forward over your foot) forces compensatory changes all the way up the kinetic chain. If the ankle can't move properly, the knee and hip pay the price. We routinely assess ankle mobility as part of any PFPS workup.
Sudden training load increases. Patellofemoral pain is fundamentally an overuse injury — the tissue is being asked to absorb more load than it can currently tolerate. This often occurs when runners ramp up their weekly mileage too quickly ahead of a race, return to running after a break, or add hills and stairs to their route without building up gradually.
Running form. Overstriding — landing with the foot well ahead of the centre of mass — dramatically increases the force through the patellofemoral joint on each step. A slightly shorter, quicker stride reduces this load considerably, and is one of the most effective biomechanical tweaks for PFPS.
How Osteopathy Treats Runner's Knee

At Back in Health Osteopathy Singapore, we take a full kinetic chain approach to PFPS. Treatment isn't limited to the knee — it addresses everything contributing to the faulty mechanics.
Gait and movement assessment. We watch you move. A single-leg squat, step-downs, and ideally a treadmill assessment of your running form reveal the biomechanical patterns that are loading your patellofemoral joint excessively. This shapes the entire treatment and rehabilitation plan.
Hip and gluteal soft tissue release. Chronically tight hip external rotators, a compressed hip joint, and trigger points in the gluteus medius and piriformis all contribute to altered lower limb mechanics. Manual soft tissue work and myofascial release in these areas begins to restore normal hip function — which is often where the most meaningful change is felt by the patient.
Lumbar and sacroiliac joint mobilisation. Restrictions in the lower back and pelvis alter how load is transferred through the hip, which in turn changes knee mechanics. Restoring mobility here is a frequently overlooked but highly effective part of PFPS treatment.
Patellar mobilisation. Gentle mobilisation of the kneecap itself — improving its ability to glide medially, laterally, and rotationally — reduces pain and restores normal tracking. This is particularly useful when the patella has been tracking laterally for a prolonged period and the surrounding tissue has adaptively tightened.
Quadriceps and IT band release. Reducing tension in the vastus lateralis and iliotibial band reduces the lateral pull on the patella and immediately decreases pain for many patients. Dry needling is highly effective for deactivating the trigger points that commonly develop in these structures in runners.
Dry needling. Back in Health offers dry needling as part of our treatment toolkit. For stubborn PFPS cases, targeted needling into the vastus lateralis, tensor fascia lata, and hip abductors can break the cycle of hypertonicity that perpetuates faulty patellar tracking.
Exercise prescription and return to running. Manual therapy alone won't prevent PFPS from returning. We prescribe a progressive strengthening programme targeting the glutes, hip abductors, and lower limb stability, and guide your return to running — including pace, gradient, surface, and volume recommendations specific to your situation. The goal is to get you back running stronger and more efficiently than before.
What You Can Do Right Now

While you're waiting for an appointment, or if your symptoms are mild and you want to start addressing the problem:
Reduce — don't necessarily stop — your running load. Complete rest often isn't needed and leads to deconditioning. Instead, reduce your weekly distance by around 30–40%, run on flat surfaces only, and avoid downhill running entirely until symptoms settle.
Start strengthening your glutes today. The most evidence-supported exercise for PFPS is hip and gluteal strengthening. Begin with clamshells, side-lying hip abduction, and single-leg glute bridges — these specifically target the muscles most commonly underactivated in runners with PFPS. Aim for daily sessions of 3 sets of 15 reps on each side.
Check your cadence. Most recreational runners overstride. Try increasing your steps per minute by around 5–10% (use a metronome app set to your current cadence plus a few BPM). This naturally shortens your stride, reduces ground reaction forces, and takes meaningful load off the patellofemoral joint.
Don't ignore the stairs. If descending stairs is painful, lead with the unaffected leg going down. This reduces the demand on the painful knee and prevents you from further irritating the joint during daily activities.
Avoid deep squats and lunges until symptoms settle. Both movements significantly increase patellofemoral compressive force. You don't need to avoid the gym entirely — upper body training, hip thrusts, and leg press with limited range are generally well tolerated — but avoid exercises that load the knee heavily in a deep bent position.
Review your training surfaces and footwear. If you've recently changed your running shoes or started running on harder surfaces (more road, less park connector), this may have contributed to the onset. A return to softer surfaces and a shoe assessment can make a meaningful difference.
When Should You See an Osteopath?
We recommend booking an assessment if:
- Knee pain during or after running has been present for more than two weeks
- Your symptoms are getting progressively worse despite reducing your training load
- Pain on stairs or after prolonged sitting is affecting your daily life
- You've tried rest and it keeps returning when you run again
- You have a race on the calendar and need a structured, evidence-based return-to-running plan
- You're unsure whether it's patellofemoral pain or something else — a proper clinical assessment matters
The earlier PFPS is properly assessed and addressed, the better the outcome. Patients who come to us within the first few weeks of onset generally recover and return to full training significantly faster than those who have been managing with rest and ice for months.
Keep Running, Singapore
Runner's knee doesn't have to end your training. It's one of the most responsive conditions we treat — when it's approached correctly. The runners who recover fastest are the ones who resist the temptation to simply rest and wait, and instead invest a few sessions in understanding and correcting the mechanics that caused the problem in the first place.
At Back in Health Osteopathy Singapore, we've helped runners at every level — from weekend Warriors doing the Bay Run to competitive athletes preparing for international events — get their knee right and get back to doing what they love.
📍 Book your assessment today at www.backinhealth.com.sg/bookings
Don't let runner's knee sideline your training. Let's find the real cause and fix it properly.
Back in Health Osteopathy Singapore offers osteopathy, IDD therapy, shockwave therapy, dry needling, and clinical pilates. To learn more about our services, visit www.backinhealth.com.sg.
This article is for general informational purposes only and does not constitute medical advice. If you are experiencing knee pain, please consult a qualified healthcare practitioner for an individualised assessment and treatment plan.
