
Understanding Disc Bulges, Sciatica, and IDD Therapy.
May 14, 2026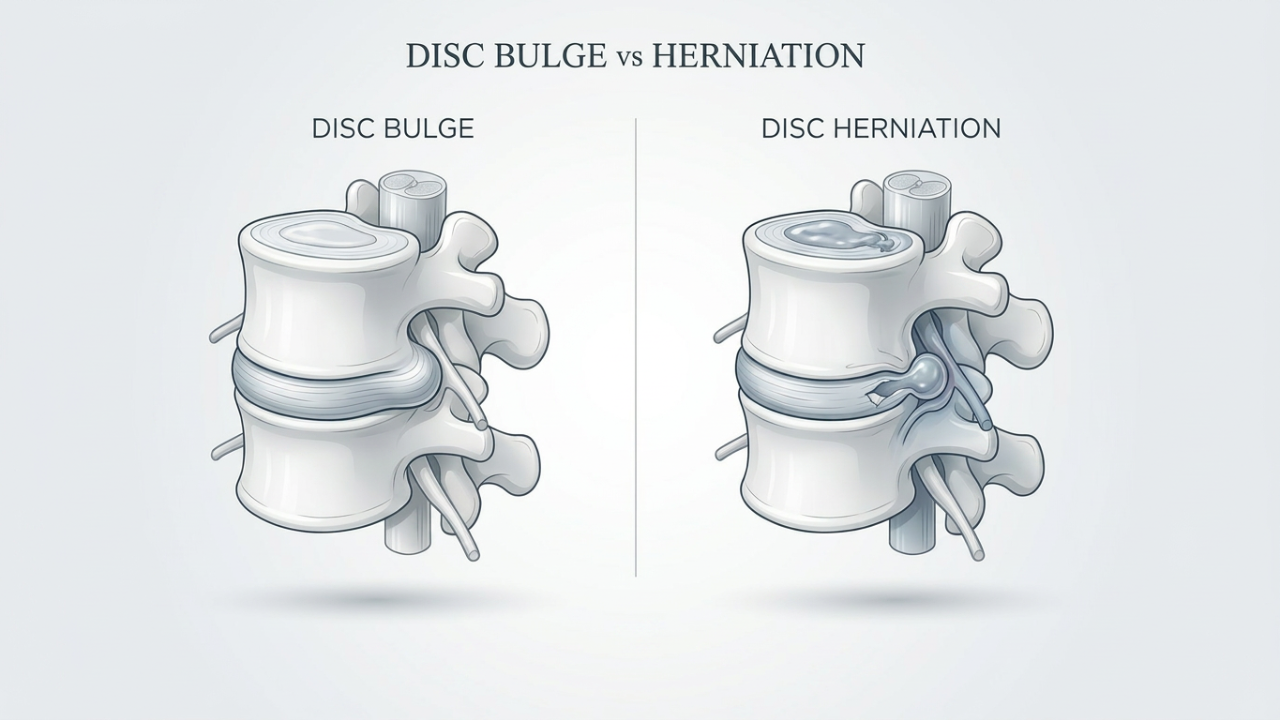
One of the biggest problems in modern spine care is that many people become frightened by MRI findings without truly understanding what those findings mean. Others are told they simply have “wear and tear” and that nothing can be done outside of medication or surgery.
The reality is far more nuanced.
Some disc injuries are relatively mild and manageable with conservative treatment. Others can create significant neurological irritation, severe pain, and substantial loss of function. Equally important, many MRI findings are poorly correlated with symptoms. A person may have a significant disc bulge and little pain, while another individual with a smaller lesion may experience substantial disability.
At Back In Health , our approach focuses not only on identifying the structural issue, but understanding how the spine is functioning mechanically, neurologically, and behaviourally as a complete system.
This article explains:
- The difference between a disc bulge and disc herniation
- Common symptoms and causes
- Why some disc injuries become chronic
- Why imaging findings do not always correlate with pain
- Conservative treatment options
- How IDD Therapy (non-surgical spinal decompression) may help appropriate patients
- The role of rehabilitation and long-term spinal resilience
Understanding the Intervertebral Disc
The intervertebral discs sit between the vertebrae of the spine and act as shock absorbers. Their role is to:
- Absorb compressive forces
- Assist movement
- Distribute load
- Maintain spacing between vertebrae
- Protect neural structures
Each disc consists of two primary structures:
Nucleus Pulposus
The soft, gel-like centre of the disc.
Annulus Fibrosus
The strong outer rings composed of collagen fibres that contain and stabilise the nucleus.
Over time, repetitive loading, poor tolerance to stress, prolonged sitting, injury, genetics, and age-related degeneration can contribute to weakening of the disc structure.
What Is a Disc Bulge?
A disc bulge occurs when the disc extends beyond its normal boundary, usually in a broad and relatively symmetrical manner.
Think of it like a tyre that is beginning to protrude slightly under pressure, but without the inner contents breaking through the outer wall.
In many cases:
- The annulus remains intact
- The bulge is broad-based
- There may be no nerve compression
- Symptoms may be mild or absent
Disc bulges are extremely common, particularly as we age.
Research has consistently shown that many asymptomatic individuals have disc bulges visible on MRI. This is important because imaging findings alone do not determine pain levels or functional limitation.
Some disc bulges are incidental findings.
Others become clinically significant.
The key question is not simply:
“Is there a bulge?”
But rather:
“Is the disc behaving as a pain generator or mechanically compromising nearby structures?”
What Is a Disc Herniation?
A disc herniation is generally more severe.
In a herniation:
- The annulus fibrosus becomes disrupted or torn
- Nuclear material pushes outward
- The disc material may compress or chemically irritate nearby nerve roots
This can create:
- Local inflammation
- Neurological irritation
- Altered movement patterns
- Protective muscle guarding
- Significant pain
Disc herniations are often categorised as:
- Protrusion
- Extrusion
- Sequestration
The severity depends on:
- Size
- Location
- Direction
- Degree of nerve involvement
- Inflammatory response
- Individual pain sensitivity
A small herniation in a sensitive location may produce more symptoms than a larger lesion elsewhere.
Common Symptoms of Disc Injury
Symptoms vary significantly depending on the location and severity of the lesion.
Lumbar Spine Symptoms
Common lower back disc symptoms include:
- Lower back pain
- Sciatica
- Gluteal pain
- Leg pain
- Numbness or tingling
- Calf or foot symptoms
- Weakness
- Difficulty standing upright
- Increased pain with sitting
- Pain during coughing or sneezing
Cervical Spine Symptoms
Neck disc injuries may produce:
- Neck pain
- Shoulder pain
- Arm symptoms
- Hand numbness
- Weakness
- Headaches
- Scapular pain
Why Some Disc Injuries Become Chronic
One of the biggest misconceptions is that pain is purely structural.
Pain is influenced by:
- Mechanical stress
- Inflammation
- Nervous system sensitivity
- Fear and avoidance
- Sleep
- Stress
- Deconditioning
- Reduced load tolerance
- Movement behaviour
Many people initially protect the injured region appropriately. However, over time this protection can become excessive.
This creates a cycle:
Pain → guarding → reduced movement → weakness → sensitivity → more pain.
At Back In Health , we frequently see patients who have become trapped in chronic protective movement strategies long after the original injury occurred.
This is why rehabilitation matters.
Reducing pain alone is not enough.
The spine must regain:
- Capacity
- Confidence
- Control
- Load tolerance
Why MRI Findings Must Be Interpreted Carefully
Modern imaging is valuable, but it also has limitations.
Research has shown that many asymptomatic individuals demonstrate:
- Disc bulges
- Degenerative changes
- Annular tears
- Facet degeneration
This means:
MRI findings must always be interpreted alongside the patient’s symptoms and clinical presentation.
Over-medicalisation of imaging findings can create unnecessary fear and catastrophisation.
Patients are often told:
- “Your spine is degenerating”
- “You have the spine of an 80-year-old”
- “Your disc is slipping out”
These explanations are often inaccurate and unhelpful.
The human spine is adaptable and resilient.
Appropriate management should focus on:
- Functional restoration
- Mechanical improvement
- Nervous system desensitisation
- Gradual return to activity
Not simply “fixing” an MRI.
Conservative Treatment Options
Most disc injuries do not require surgery.
Conservative management may include:
- Osteopathic treatment
- Physiotherapy
- Exercise rehabilitation
- Strength and conditioning
- Activity modification
- Education
- Dry needling
- Shockwave therapy
- Medication when appropriate
- Spinal decompression approaches
The challenge is that not all treatments address the mechanical loading environment of the disc itself.
This is where spinal decompression approaches such as IDD Therapy may play a role.
What Is IDD Therapy?
IDD Therapy stands for Intervertebral Differential Dynamics Therapy.
It is an advanced form of non-surgical spinal decompression designed to target specific spinal segments in a controlled and progressive manner.
Unlike traditional traction, IDD Therapy:
- Uses computer-controlled treatment protocols
- Targets specific spinal levels
- Gradually increases tolerance
- Incorporates oscillation and controlled force progression
- Aims to reduce protective muscular guarding
- Allows patients to relax during treatment
At Back In Health , IDD Therapy is commonly integrated alongside rehabilitation and manual therapy rather than used in isolation.
How IDD Therapy May Help Disc Injuries
The proposed goals of IDD Therapy include:
- Reducing compressive loading on the disc
- Creating decompression forces
- Improving movement at restricted spinal segments
- Reducing muscle spasm and guarding
- Improving patient tolerance to movement
- Assisting symptom reduction
Some patients report:
- Reduced leg symptoms
- Improved standing tolerance
- Reduced stiffness
- Improved mobility
- Improved function
Clinically, the most appropriate patients are often those with:
- Persistent disc-related symptoms
- Mechanical back pain
- Sciatica
- Cervical radiculopathy
- Chronic compressive spinal loading patterns
- Failure to improve with standard conservative care alone
IDD Therapy Is Not a Miracle Cure
This is important.
No legitimate clinician should claim that spinal decompression “puts discs back in place” or permanently “fixes” every disc injury.
That is oversimplified marketing.
Disc injuries are multifactorial.
Successful outcomes usually involve:
- Mechanical unloading
- Improved movement behaviour
- Progressive rehabilitation
- Load management
- Strength restoration
- Lifestyle modification
- Nervous system desensitisation
IDD Therapy should be viewed as:
A tool within a comprehensive management strategy.
Not a stand-alone magic solution.
The Importance of Rehabilitation After Disc Injury
Pain reduction alone is not sufficient.
If the patient:
- Remains weak
- Avoids movement
- Has poor endurance
- Cannot tolerate load
- Has poor spinal control
…the risk of recurrence remains high.
At Back In Health , rehabilitation often focuses on:
- Controlled movement exposure
- Trunk capacity
- Hip strength
- Walking tolerance
- Breathing and bracing strategies
- Progressive loading
- Functional strength
The goal is not simply symptom relief.
The goal is restoring human capacity.
When Surgery May Be Necessary
While many patients improve conservatively, surgery may be appropriate in some cases.
Urgent medical assessment is important if symptoms include:
- Progressive neurological weakness
- Loss of bowel or bladder control
- Saddle numbness
- Severe progressive neurological compromise
- Significant loss of function
These may indicate serious neurological involvement requiring immediate medical attention.
Our Clinical Perspective
One of the biggest problems in spine care is over-simplification.
Patients are often pushed into one of two extremes:
- “Nothing is wrong”
or - “You need surgery immediately”
The reality usually lies somewhere in between.
At Back In Health , our philosophy is centred around:
- Careful assessment
- Clinical reasoning
- Individualised management
- Progressive rehabilitation
- Long-term resilience
Disc injuries are rarely just about the disc itself.
They involve:
- The nervous system
- Movement behaviour
- Fear and confidence
- Physical capacity
- Stress adaptation
- Mechanical tolerance
Successful recovery often requires addressing all of these components together.
Frequently Asked Questions
Can a disc bulge heal naturally?
Many disc injuries improve significantly over time, particularly with appropriate management, gradual movement exposure, and rehabilitation.
Is a disc bulge permanent?
Some imaging findings may remain visible even after symptoms improve. Pain and MRI findings do not always correlate directly.
Is surgery always required for disc herniation?
No. Many disc herniations improve with conservative care.
Is IDD Therapy painful?
Most patients tolerate IDD Therapy well. Treatment is designed to be gradual and controlled.
How many IDD sessions are usually required?
This varies depending on the severity and chronicity of the condition. Structured programs are commonly recommended to achieve cumulative effects.
What is the difference between traction and IDD Therapy?
Traditional traction is generally more generic and less targeted. IDD Therapy uses computer-controlled protocols designed to target specific spinal segments progressively.
Can exercise make a disc injury worse?
Poorly selected or excessive loading may aggravate symptoms. However, appropriate exercise is usually an important part of recovery.
Should I stop exercising completely?
In most cases, complete inactivity is not recommended. Appropriate movement is often beneficial.
Can MRI scans predict pain levels?
Not reliably. Many asymptomatic individuals have significant MRI findings.
Final Thoughts
Disc bulges and disc herniations are common, but they are often misunderstood.
Imaging findings alone do not determine outcomes.
Pain is rarely purely structural.
And surgery is not the only pathway.
Appropriate conservative management may help many individuals improve function, reduce pain, and regain confidence in movement.
For some patients, IDD Therapy may offer an additional option within a broader rehabilitation strategy aimed at reducing compressive spinal loading and improving mechanical tolerance.
The key is not simply chasing pain relief.
The goal should be restoring resilience, movement confidence, and long-term spinal capacity.
Categories
All Categories acupuncture acute traumatic muscle pain adhesive capsulitis alternative medicine alternative therapy anterior knee pain baby osteopathy back care back exercises back in health osteopathy back in health singapore back pain back pain relief back stretches balance body balance breastfeeding issues bukit timah trail running carpal tunnel surgery carpal tunnel syndrome cervicogenic headache child health children’s osteopath chiropractic chiropractor chiropractor singapore chronic headaches chronic overuse muscle pain chronic pain clinical pilates clinical strength and conditioning colic relief conditioning classes core strength core strengthening cranial osteopathy cts treatment developmental support difference between osteopath and chiropractor doms dry needling endurance training ergonomics eswt exercise therapy extracorporeal shock wave therapy family wellness fitness fitness classes flexibility frozen shoulder frozen shoulder treatment functional training gentle therapy growing pains hand numbness hand pain headache relief singapore headaches headaches and migraines healthcare professionals herniated disc holistic holistic headache treatment holistic health holistic healthcare holistic treatment home remedies for headaches hydration idd therapy idd therapy near me infant osteopath injury prevention joint pain knee pain going downstairs knee pain running knee pain singapore knee pain when running singapore leg pain lower back exercises lower back pain lumbar pain manual therapy marathon singapore massage therapy mat pilates median nerve migraine clinic singapore migraine relief migraine treatment mindful movement mobility mobility training movement therapy muscle cramps muscle guarding muscle knots muscle pain muscle recovery muscle spasms muscle strain muscle tension musculoskeletal care musculoskeletal health musculoskeletal pain myofascial trigger points natural headache remedies natural healing neck pain neck pain and headache neck pain from desk work neck pain singapore neck pain treatment singapore nerve compression nerve pain newborn care non-invasive therapy orthopaedic therapy osteopath osteopath for neck pain osteopath singapore osteopath vs chiropractor osteopathic treatment osteopaths near me osteopaths singapore osteopathy osteopathy for migraines overuse injuries paediatric osteopath paediatric treatment pain management pain relief park connector running patellofemoral pain patellofemoral pain syndrome singapore pediatric osteopathy personal training physical therapy physiotherapy pilates pilates classes pilates for back pain pilates singapore pilates studio plantar fasciitis posture correction reformer pilates rehabilitation rehabilitation exercises repetitive strain injury rice principle rotator cuff rotator cuff injury singapore rotator cuff treatment singapore rotator cuff without surgery singapore rsi runner's knee singapore runner's knee symptoms runner's knee treatment singapore running injury singapore sciatica sciatica relief sciatica treatment shockwave shockwave benefits shockwave for athletes shockwave singapore shockwave therapy shoulder exercises shoulder impingement singapore shoulder injury shoulder mobility shoulder pain shoulder pain osteopathy shoulder pain treatment singapore shoulder rehabilitation shoulder stiffness singapore singapore idd therapy singapore runners sleep improvement slipped disc soft tissue therapy spinal alignment spinal decompression treatment spinal health spine alignment spine health sports injuries sports injury recovery sports performance stiff shoulder strength building strength training stretching sundown marathon tech neck tendon healing tendonitis tension headache text neck theatre sign knee tingling fingers tissue healing treatment trigger point therapy underuse syndrome warm-up wellness wellness singapore wrist care wrist exercises wrist pain wrist splint